-
-
It's not 5AR2, it's DHT. Oral medications like finasteride and dutasteride work that well because they actually decrease serum DHT. I don't exactly understand what you mean by "spillover"?
if you are going to only inhibit 5AR2 at scalp level you ain't going to get far because sufficient DHT will still be produced at other sites in the body. This will go into circulation and will attach to the DP AR through the blood. I think your heart pumps your blood around not ?
?
We can actually also understand this as on the scalp 5AR1 expression is way more prevalent and expressed in the scalp;
As you know finasteride has no effect on 5AR1. Furthermore highly contradicting studies are found about 5AR2 in terms of the micro environment of the hair follicle. Some older studies say that 5AR2 expression is found in the dermal papilla but some later studies show that 5AR2 expression is minimal there to non existent. For instance a recent one;The predominant form of 5alpha-reductase (5aR) in human scalp is 5aR1.
Anyway if "local" activity was such a predominant factor then why does finasteride work in most people while 5AR1 is by far the most active enzyme in the scalp? Can you explain? Considering that finasteride has no impact on 5AR1?Abstract: Androgens regulate hair growth, and 5alpha-reductase (5alphaR) plays a pivotal role in the action of androgens on target organs. To clarify the molecular mechanisms responsible for controlling hair growth, the present study presents evidence that the human follicular dermal papilla cells (DPCs) from either beard (bDPCs) or scalp hair (sDPCs) possess endogenous 5alphaR activity. Real-time RT-PCR revealed that the highest level of 5alphaR1 mRNA was found in bDPCs, followed by sDPCs, and a low but detectable level of 5alphaR1 mRNA was observed in fibroblasts. Minimally detectable levels of 5alphaR2 mRNA were found in all three cell types.
Also on a genetical level there is really nothing in terms of the 5-reductases in terms of the pathology of androgenetic alopecia. The androgen receptor is.
Local androgen receptor blocking would be enough, local 5-reductase blocking would be not. Simply because DHT is still being produced at other local sites, and the DHT will still find it's way to the dermal papilla. If you block the androgen receptor however DHT will never bind to the hair follicle.
That is why topical AR antagonists with a good safety profile are so much more exciting than finasteride.
Anyway topical finasteride will go systemic, there is no other way around and there are no magical vehicles. The dose response curve as mentioned here by FTL is a factor and metabolism of the compound can't occur quickly enough before going systemic.Comment
-
Comment
-
I understand that DHT carried through the blood will still eat at the hair follicle; but I don't mind experimenting to see if eliminating the DHT locally can at least help to slow down the loss until something better comes out. I am going through the recession process and I want to try applying some creamy fin on my hairline before bed rather than going all out with the pill; I don't need help in the crown or any other area.
Having said that; my hair responded really well to .25mg of oral fin everyday. What concentration and vehicle should I ask for at the compounding pharmacy to attain an equivalent effect with the topical? Is anyone here knowledgeable enough about this or should I just ask the pharmacist?
Thanks guysComment
-
Can you send the formula? I know how to get it done. Thanks much.Comment
-
Isnt DHT in the scalp or converted to DHT in the scalp? I don't know the mechanism. You are saying systemically Finasteride blocks the conversion of Testosterone to DHT in the blood? I thought this occurs in different organs of the body, ie, testicles, skin. Can you help me out?Comment
-
First do an internet search. Someone here should know the concentration recommended.
Having said that consider this: if you have Finasteride 1% soln then that means you hav 1000mg/100ml or 10mg/ml. The question now is how much is systemically absorbed? I don't know but if I was making a solution and want to use 2 X 1ml I might make 0.1% solution. You do the math, 1.0mg/ml with the assumption there was somewhere around a 70% absorption. This is all theory so don't go make a 0.5% and use because it may be too much.
I just want you to know concentrations, absorption considerations and I would dissolve in Minoxidil soln, perfect hydro-alc-peg solvent
If you make your own and don't want the powder fillers in your solution, make up 30-60ml solution dissolved in Minox or other and pass it thru a coffee filter. Wet the filter first with Isopropyl Alc 70% so no drug sticks to the filter. I highly recommend 100ml graduate cylinder to do your prepping bought on line or your local INDEPENDENT pharmacy will get you one. Does this help anyone?Comment
-
Yeah you could be right. I actually hope that CB proves to be very potent and have a good side effect profile. Perhaps CB could be used indeed at a high concentration to almost shield of all DHT from the androgen receptors + test. I guess we will have to wait on the study results to see how CB really behaves. Hopefully they will release much information after the clinical trial completion.Comment
-
I disagree, I believe oral medications like the above work because they reduce DHT in the target tissue, not due to systemic reduction. For spillover, I will attempt to explain. Rough analogy - So in the walls and in the tower cables outside you have alternating current being transported everywhere. Upon reaching your house though, that AC has to be converted to DC before it is used in your appliances. Similarly, T floats around in your body, but in certain tissues, for it to be effective, T needs to enter the relevant cells, be converted to DHT which in turn will do what it is supposed to. Some of that DHT will of course leave the cell and enter the bloodstream, and I believe it is this spillover that systemic DHT levels typically show.
Heart pumps blood around, sure, but serum DHT levels are TINY compared to T levels.
That's the thing, the scalp is NOT the target tissue here! The target tissue is the hair follicle, more specifically the dermal papilla. Which 5AR isoform is present in the DP? Of course type 2. That is why fin is effective, it shuts down DHT selectively. An AR blocker would a much more "blunt" instrument compared to a 5AR2 inhibitor.
This is why topical finasteride does not need to go systemic to work. If you are correct, then a systemic 5AR1 inhibitor will also work? I am skeptical though.Comment
-
If DHT from adjacent tissues was more important, then given that 5AR1 is more prevalent in the scalp, presumably it would override the 5AR2 inhibition.Comment
-
As far as I know Merck did a study on balding stumptail macaque with the drug MK386 which is a 5AR1 inhibitor and it wasn't effective. However it only reduced -30% serum DHT in the monkeys. Heck of a lot less than the average of what like -70% of finasteride? Finasteride did work in the monkeys
Look at this study though;

So in this study they actually state that the 5AR1 type is more expressed in DPC than 5AR2. Finasteride doesn't really have much impact on 5AR1. So isn't that strange in combination with the monkey observations? Assuming that a stumptail macaque is a good model? Why did finasteride then show to be effective in the monkey and the 5AR1 specific inhibitor did not? Keep in mind that the expression of 5AR1 is higher in this study in DPC.
Check the following study; http://www.hormones.gr/49/article/article.html. As stated;
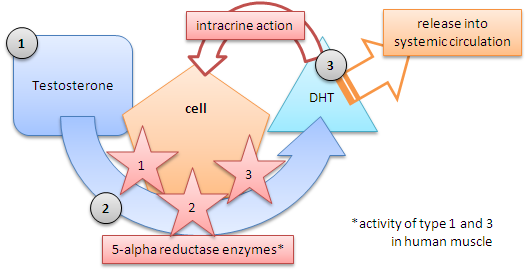
So it's definitely a thing that many cell types which express 5AR work in a endocrine manner and so release the DHT into circulation. How do we know that the dermal papilla actually doesn't work in a endocrine manner? Or does it work intracrine? Or a combination if that is possible(?)? I personally think it's intracrine but have trouble really finding literature on this.DHEA and androstenedione are converted to testosterone and further to 5α-DHT by the intracellular enzyme 5α-reductase in skin, thus making the skin a source of considerable amounts of the circulating testosterone and 5α-DHT levels.
Let's assume though that 5AR2 is only expressed in DPC and the above study is flawed. Besides that the dermal papilla cells only work in a intracrine manner. Even then I do believe that serum DHT can/will have impact. Simply because when you block locally or only at the DPC enough cells are still working in a endocrine fashion and that still leaves a shitload of serum DHT. This will bind to the AR DPC.
It would be great to see how much local 5AR2 activity blocking would have merit if we would actually have a compound that blocks 5AR2 locally without going systemic and thus reducing serum DHT. Unfortunately as showed by several studies finasteride topically does reduce serum DHT and there is no way around it.
Personally I think local blocking would be effective but surely less effective than systemic blocking.Comment
-
This thread is a waste of time. I have tried topical fin in many different formulations and dosages and the same sides as oral fin surface. This is because of the dose response curve for the drug. It will go systemic, and even a little bit will cause sides for people who are prone to fin sides.
End of topic.Comment

 Tweet
Tweet





Comment