-
No, but I am willing to give it a shot. Would be at least a year before I could discern any results anyway. I have .25mg doses all cut up and ready to go. Jazz is a big believer in taking .25 eod. -
So, it looks like taking around .25mg or .50mg of Fin once a week is the perfect amount to drop your DHT levels while still allowing your body to use its mechanisms to recover... Maybe one of the issues with fin is that by taking it everyday we compound its effects to the point where the body is so overwhelmed and forced into hypogonadism ?
Anyone tried microdosing like that?Leave a comment:
-
I see maybe your right that it always goes nearly 100 percent systemic. Maybe that is why merk gave men the choice on topical or oral formulation. Other than convenience there is not much of a difference in terms of sides I guess.
Kind of a shame that is the case, but it is what it is.Leave a comment:
-
-
No problem guys, sorry for the delay. I am posting it as we speak
Hi brother It is a topical foaming solution, similar to the Regain foam (Minoxidil) available on the market.
It is a topical foaming solution, similar to the Regain foam (Minoxidil) available on the market.
The first batch is ready tomorrow for a patient. I am making one for myself as well. I'll keep you posted on efficacy, etc
Leave a comment:
-
Topical finasteride goes pretty much almost 100% systemic;
Comparing the therapeutic effects of finasteride gel and tablet in treatment of the androgenetic alopecia.
Hajheydari Z1, Akbari J, Saeedi M, Shokoohi L.
Author information
Abstract
BACKGROUND:
Finasteride, a type II-selective 5alpha-reductase inhibitor, as a causative agent of decreasing dihydroxy testosterone (DHT) level, is effective in the treatment of male androgenic alopecia.
AIM:
We compared the local and oral finasteride in the treatment of androgenic alopecia.
METHOD:
This is a double blind, randomized clinical trial study of 45 male patients, who were referred with alopecia to the private clinics and departments in Boo-Ali Sina Hospital, in Sari. Patients with male androgenic alopecia were selected according to the history and physical examinations. The patients were randomly divided into two: topical finasteride (A) and oral finasteride (B) groups. Topical finasteride group (A) received a topical gel of 1% finasteride and placebo tablets, while the oral finasteride group (B) received finasteride tablets (1 mg) and gel base (without drug) as placebo for 6 months. The patients were followed by clinical observation and recording of side effects prior to the treatment and at the end of first week, and then by a monthly follow-up. The size of bald area, total hair count, and terminal hair were studied. Data were analyzed by descriptive and Chi-square statistical test.
RESULTS:
The mean duration of hair loss was 18.8+/-23.10 months. Each month the terminal hair, size of bald area and hair count between the two groups were compared. There were no significant differences between the two groups as a viewpoint of hair thickness, hair counts and the size of bald area. Serial measurements indicated a significant increase in hair counts and terminal hair counts between the two groups.
CONCLUSIONS:
The results of this study showed that the therapeutic effects of both finasteride gel and finasteride tablet were relatively similar to each other.Pharmacodynamic of P-3074 (finasteride 0.25% topical solution) in subjects with androgenetic alopecia
A new proprietary topical formulation, P-3074, containing finasteride 0.25% as active ingredient and hydroxypropyl-chitosan (HPCH) as film-forming agent, was developed for androgenetic alopecia. The present study was aimed at investigating the pharmacodynamic profile of finasteride in terms of dihydrotestosterone (DHT) concentrations in the scalp and in serum after multiple topical application of P-3074 or oral finasteride intake in subjects with androgenetic alopecia. Eighteen healthy men were randomly allocated to P-3074 or oral treatment after providing written informed consent. Twelve volunteers applied P-3074 topical solution for 7 days: six subjects once daily (o.d.) in the morning and the others twice daily (b.i.d.) in the morning and in the evening. The third group of six volunteers was administered 1 mg oral finasteride once daily in the morning for 1 week. Scalp (vertex) biopsies were collected at baseline and 6 hours after last dose administration, while serum samples were collected at baseline, before last administration, and 6 and 12 hours after the last multiple dose. A marked decrease in scalp DHT levels was observed: by 47.22% with P-3074 b.i.d., from 1.91 (�0.54) to 1.01 ng ml−1 (�0.39), by 71.20% with P-3074 o.d., from 1.52 (�0.41) to 0.44 ng ml−1 (�0.08), and by 51.11% with the oral formulation, from 1.39 (�0.25) to 0.68 ng ml−1 (�0.34). Serum DHT was reduced by 69.3�74.0% with P-3074 b.i.d., 67.6�80.4% with P-3074 o.d., and 69.7�76.1%with the oral formulation. These results showed a similar inhibition of serum DHT after 1 week of finasteride administration with the three dose regimens and were consistent with the results obtained in a previous P-3074 PK study. These findings show that DHT concentration in the scalp, after 7-day treatment course of P-3074 o.d., was more reduced (about 40%) than after 1 mg oral finasteride administration for the same treatment period.Leave a comment:
-
combined with half life, theres no way around the sidesLeave a comment:
-
I think the question is just to what degree does it go systemic topically? We all acknowledge it probably does but less is always better than more if it can be effective still locally near the hair.
I remember bryan mentioning that 5-ar 1 inhibitor before. If 5-ar 1 is found mainly in the skin and type 2 isnt then its possible for type 1 the skin plays more a role their with DHT production than it does with finasteride where its other places like prostate where its more common. Its always been the 5-ar type 2 implicated in MPB and not so much the type 1 which I admit is odd since type 1 is more abundant local to hair cells supposedly.Leave a comment:
-
Well having an AR antagonist which doesn't go systematically would surely kick a**? I guess the problem is I wouldn't even want a small amount of something like spiro going systematically.Leave a comment:
-
This thread is a waste of time. I have tried topical fin in many different formulations and dosages and the same sides as oral fin surface. This is because of the dose response curve for the drug. It will go systemic, and even a little bit will cause sides for people who are prone to fin sides.
End of topic.Leave a comment:
-
-
As far as I know Merck did a study on balding stumptail macaque with the drug MK386 which is a 5AR1 inhibitor and it wasn't effective. However it only reduced -30% serum DHT in the monkeys. Heck of a lot less than the average of what like -70% of finasteride? Finasteride did work in the monkeys
Look at this study though;

So in this study they actually state that the 5AR1 type is more expressed in DPC than 5AR2. Finasteride doesn't really have much impact on 5AR1. So isn't that strange in combination with the monkey observations? Assuming that a stumptail macaque is a good model? Why did finasteride then show to be effective in the monkey and the 5AR1 specific inhibitor did not? Keep in mind that the expression of 5AR1 is higher in this study in DPC.
Check the following study; http://www.hormones.gr/49/article/article.html. As stated;
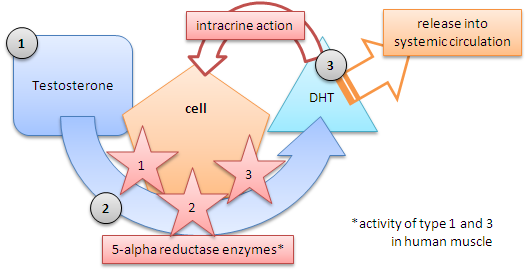
So it's definitely a thing that many cell types which express 5AR work in a endocrine manner and so release the DHT into circulation. How do we know that the dermal papilla actually doesn't work in a endocrine manner? Or does it work intracrine? Or a combination if that is possible(?)? I personally think it's intracrine but have trouble really finding literature on this.DHEA and androstenedione are converted to testosterone and further to 5α-DHT by the intracellular enzyme 5α-reductase in skin, thus making the skin a source of considerable amounts of the circulating testosterone and 5α-DHT levels.
Let's assume though that 5AR2 is only expressed in DPC and the above study is flawed. Besides that the dermal papilla cells only work in a intracrine manner. Even then I do believe that serum DHT can/will have impact. Simply because when you block locally or only at the DPC enough cells are still working in a endocrine fashion and that still leaves a shitload of serum DHT. This will bind to the AR DPC.
It would be great to see how much local 5AR2 activity blocking would have merit if we would actually have a compound that blocks 5AR2 locally without going systemic and thus reducing serum DHT. Unfortunately as showed by several studies finasteride topically does reduce serum DHT and there is no way around it.
Personally I think local blocking would be effective but surely less effective than systemic blocking.Leave a comment:
-
If DHT from adjacent tissues was more important, then given that 5AR1 is more prevalent in the scalp, presumably it would override the 5AR2 inhibition.Leave a comment:
-
I disagree, I believe oral medications like the above work because they reduce DHT in the target tissue, not due to systemic reduction. For spillover, I will attempt to explain. Rough analogy - So in the walls and in the tower cables outside you have alternating current being transported everywhere. Upon reaching your house though, that AC has to be converted to DC before it is used in your appliances. Similarly, T floats around in your body, but in certain tissues, for it to be effective, T needs to enter the relevant cells, be converted to DHT which in turn will do what it is supposed to. Some of that DHT will of course leave the cell and enter the bloodstream, and I believe it is this spillover that systemic DHT levels typically show.
Heart pumps blood around, sure, but serum DHT levels are TINY compared to T levels.
That's the thing, the scalp is NOT the target tissue here! The target tissue is the hair follicle, more specifically the dermal papilla. Which 5AR isoform is present in the DP? Of course type 2. That is why fin is effective, it shuts down DHT selectively. An AR blocker would a much more "blunt" instrument compared to a 5AR2 inhibitor.
This is why topical finasteride does not need to go systemic to work. If you are correct, then a systemic 5AR1 inhibitor will also work? I am skeptical though.Leave a comment:









Leave a comment: