 Tweet
Tweet
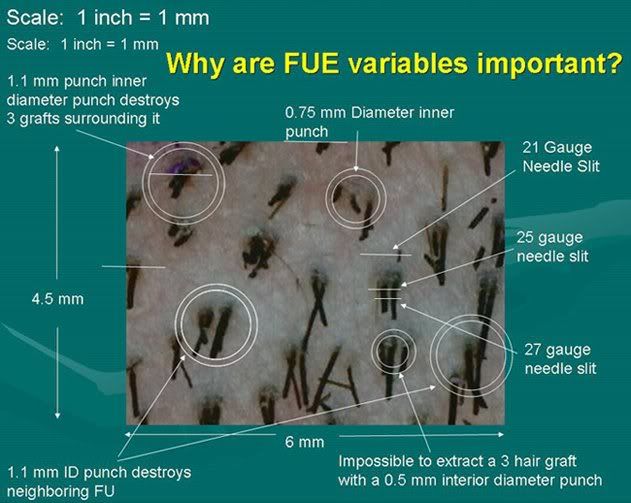
Guys, trust me, the difference between 1 mm and .95 mm is not that much in the right hands. A manual extraction with a .95 mm punch however can potentially show more scarring, and do more collateral damage than a 1mm robotic punch precisely placed.
The real issue IMHO is that the potential collateral damage done with manual extractions far exceed the potential damage of robotic extractions which IMHO are today now far more accurate. Why? You have more control over the torsion, traction, and compression issues that vary quite a bit between the proficiencies of various docs' skill levels when they manually extract.
Yet I do still agree that more refinements and experience have a ways to go and yet we must not forget the element of potential transection of the grafts and why the open-ended risk of manual extraction skills varies throughout the industry between the doctors.
That is why the yields with manual FUE still vary to this day.
The real issue IMHO is that the potential collateral damage done with manual extractions far exceed the potential damage of robotic extractions which IMHO are today now far more accurate. Why? You have more control over the torsion, traction, and compression issues that vary quite a bit between the proficiencies of various docs' skill levels when they manually extract.
Yet I do still agree that more refinements and experience have a ways to go and yet we must not forget the element of potential transection of the grafts and why the open-ended risk of manual extraction skills varies throughout the industry between the doctors.
That is why the yields with manual FUE still vary to this day.








Comment