-
 links to autoimmune disease links to autoimmune disease
I was just reading up on MPB and what causes it, and there are definitely links to autoimmune disorders.
Mast cells are one interesting aspect. They are shown to exist in much higher numbers in bald scalp. Mast cells exist next to the hair follicle, and interact with hair follicle cells. They are basically cells that release histamines and other things(which in turn cause an allergic inflammatory reaction, and also cause fibrosis) Mast cells also release PGD2 and serotonin (SSRI drugs, which keep more serotonin in the bloodstream, have been implicated in hair loss as a side effect). PGD2 we all know also causes hair loss.
"Mast cells may be implicated in the pathology associated with autoimmune, inflammatory disorders of the joints. They have been shown to be involved in the recruitment of inflammatory cells to the joints (e.g., rheumatoid arthritis) and skin (e.g., bullous pemphigoid), and this activity is dependent on antibodies and complement components.[19]"
This is probably why Replicel's healthy DSC cells work for tendonitis. They somehow reduce mast cell activity or release factors that do the opposite of histamines and other molecules.
There's also something going on with alcohol and baldness. It's been proven that homeless alcoholic men have less incidence of baldness (i see evidence of it every day). EtOH (ethanol) has been shown to bind with the androgen receptor. Also, finasteride has been shown to reduce cravings for alcohol. One theory is that finasteride reduces the production of neurosteroids, which cause cravings for alcohol. Steroids like hydrocortisone also bind to the androgen receptor and reduce inflammation. Maybe alcoholic men tend to have more neurosteroids and thus their androgen receptors are less prone to connect to DHT?? Either way it all points back to the immune response again. DHT causes hair follicle cells to produce MHC II cells, which in turn facilitate the recognition of antigens by T cell receptor sites on cells. (antigens tell the body to destroy cells, such as hair cells). In alopecia areata, T cells destroy the hair follicle. Is it possible that in MPB, T Cells are also implicated? Or maybe it is the mast cells that are forced into action by the MHC II cells. Mast cells and T cells are known to communicate and activate each other. Either way, it seems that an immune system related reaction is what causes the follicle to undergo apoptosis.
I think Christiano is on the right track, but maybe there's something missing in the puzzle. I think drugs like CB that bind to the androgen site or finasteride which reduces the amount of DHT made are only working on the outermost layer of the problem. I don't think PGD2 blockers are the answer, because PGD2 is only one element that causes this immune response. It seems to me that a permanent cure lies in reprogramming the hair cells to break their communication with the immune response. What is the antigen involved in MPB? Is there one?
I think that a topical version of what they are suing in Areata could in fact help in suppressing MPB. I'm curious for someone to try it. The problem is that with MPB, androgens keep telling the hair cells to activate the genes that cause this similar immune response, whereas in Areata, they are basically fixing the "trigger". Maybe the ultimate answer for MPB is a similar fix of the immune response combined with a blocking of the androgen receptor. I'm really curious to know what researchers have to say about all this.
On a side note- I wonder if Christiano has looked into the same drugs in order to treat Vitiligo. It seems that skin discoloration is also caused by these same autoimmune issues. I bet that if they administered the drug to vitiligo patients it would have a positive effect. just a guess.
This news also seems very related and relevant, and I wonder if it can be applied to MPB as well:
http://www.bris.ac.uk/news/2014/sept...e-disease.html
-
 Originally Posted by sdsurfin

I was just reading up on MPB and what causes it, and there are definitely links to autoimmune disorders.
Mast cells are one interesting aspect. They are shown to exist in much higher numbers in bald scalp. Mast cells exist next to the hair follicle, and interact with hair follicle cells. They are basically cells that release histamines and other things(which in turn cause an allergic inflammatory reaction, and also cause fibrosis) Mast cells also release PGD2 and serotonin (SSRI drugs, which keep more serotonin in the bloodstream, have been implicated in hair loss as a side effect). PGD2 we all know also causes hair loss.
"Mast cells may be implicated in the pathology associated with autoimmune, inflammatory disorders of the joints. They have been shown to be involved in the recruitment of inflammatory cells to the joints (e.g., rheumatoid arthritis) and skin (e.g., bullous pemphigoid), and this activity is dependent on antibodies and complement components.[19]"
This is probably why Replicel's healthy DSC cells work for tendonitis. They somehow reduce mast cell activity or release factors that do the opposite of histamines and other molecules.
There's also something going on with alcohol and baldness. It's been proven that homeless alcoholic men have less incidence of baldness (i see evidence of it every day). EtOH (ethanol) has been shown to bind with the androgen receptor. Also, finasteride has been shown to reduce cravings for alcohol. One theory is that finasteride reduces the production of neurosteroids, which cause cravings for alcohol. Steroids like hydrocortisone also bind to the androgen receptor and reduce inflammation. Maybe alcoholic men tend to have more neurosteroids and thus their androgen receptors are less prone to connect to DHT?? Either way it all points back to the immune response again. DHT causes hair follicle cells to produce MHC II cells, which in turn facilitate the recognition of antigens by T cell receptor sites on cells. (antigens tell the body to destroy cells, such as hair cells). In alopecia areata, T cells destroy the hair follicle. Is it possible that in MPB, T Cells are also implicated? Or maybe it is the mast cells that are forced into action by the MHC II cells. Mast cells and T cells are known to communicate and activate each other. Either way, it seems that an immune system related reaction is what causes the follicle to undergo apoptosis.
I think Christiano is on the right track, but maybe there's something missing in the puzzle. I think drugs like CB that bind to the androgen site or finasteride which reduces the amount of DHT made are only working on the outermost layer of the problem. I don't think PGD2 blockers are the answer, because PGD2 is only one element that causes this immune response. It seems to me that a permanent cure lies in reprogramming the hair cells to break their communication with the immune response. What is the antigen involved in MPB? Is there one?
I think that a topical version of what they are suing in Areata could in fact help in suppressing MPB. I'm curious for someone to try it. The problem is that with MPB, androgens keep telling the hair cells to activate the genes that cause this similar immune response, whereas in Areata, they are basically fixing the "trigger". Maybe the ultimate answer for MPB is a similar fix of the immune response combined with a blocking of the androgen receptor. I'm really curious to know what researchers have to say about all this.
On a side note- I wonder if Christiano has looked into the same drugs in order to treat Vitiligo. It seems that skin discoloration is also caused by these same autoimmune issues. I bet that if they administered the drug to vitiligo patients it would have a positive effect. just a guess.
This news also seems very related and relevant, and I wonder if it can be applied to MPB as well:
http://www.bris.ac.uk/news/2014/sept...e-disease.html
searching google (typing mast cells t cell) there seams to be a strong correlation between the two. an example :T cell-induced mast cell activation: a role for microparticles released from activated T cells. and the JAK inhibitor they tested suppresses t-cells. so it might work in different pathways.
1- as an anagen promoter via activation of hair follicle stem cells.
2- supressing t-cells -> suppressing mast cells-> inhibiting PGD2.
-
Originally Posted by hgs1989
searching google (typing mast cells t cell) there seams to be a strong correlation between the two. an example :T cell-induced mast cell activation: a role for microparticles released from activated T cells. and the JAK inhibitor they tested suppresses t-cells. so it might work in different pathways.
1- as an anagen promoter via activation of hair follicle stem cells.
2- supressing t-cells -> suppressing mast cells-> inhibiting PGD2.
This is an interesting article as well: https://groups.google.com/forum/#!to...on/dRvFNzZj7ks
seems MPB is definitely part of an immune system reaction. I really hope they figure this shit all out, it seems like we are so close to knowing exactly why it happens. Maybe they could already know if they pieced all the parts together. Also, Christiano mentions in her patent that the JAK inhibitor works very differently as a topical in mice than when it is used systemically. I wonder if its the same in humans. It seems to work systemically for areata, but maybe for MPB it needs to be topical or more focused on the hair follicle cells. I think that the patent hints at targeting hair follicle cells with this stuff but I'm not sure. I hope for big revelations in the near future.
-
Originally Posted by sdsurfin
This is an interesting article as well: https://groups.google.com/forum/#!to...on/dRvFNzZj7ks
seems MPB is definitely part of an immune system reaction. I really hope they figure this shit all out, it seems like we are so close to knowing exactly why it happens. Maybe they could already know if they pieced all the parts together. Also, Christiano mentions in her patent that the JAK inhibitor works very differently as a topical in mice than when it is used systemically. I wonder if its the same in humans. It seems to work systemically for areata, but maybe for MPB it needs to be topical or more focused on the hair follicle cells. I think that the patent hints at targeting hair follicle cells with this stuff but I'm not sure. I hope for big revelations in the near future.
Now ask yourself this:
Why in the hell has not a single doctor tried a JAK inhibitor for AGA either orally or topically?
-
Originally Posted by sdsurfin
I was just reading up on MPB and what causes it, and there are definitely links to autoimmune disorders.
Great analysis and very interesting, thanks for this.
-
Thanks interesting story. Although I do think they have similarities, I think AGA primarily isn't a autoimmune disease though.. If it was we would see way more reversal of AGA just as with alopecia aerata. Well maybe sort of a auto-immune disease I would like to call it a protect mechanism. I think that Michael Philpott (I think that is his name) is right in his assumption that this is a sort of fast forward "aging" state driven by ROS/oxidative stress (DHT YOU B*TCH) I think P53 has a huge role as seen in this diagram, I always like to post this one;
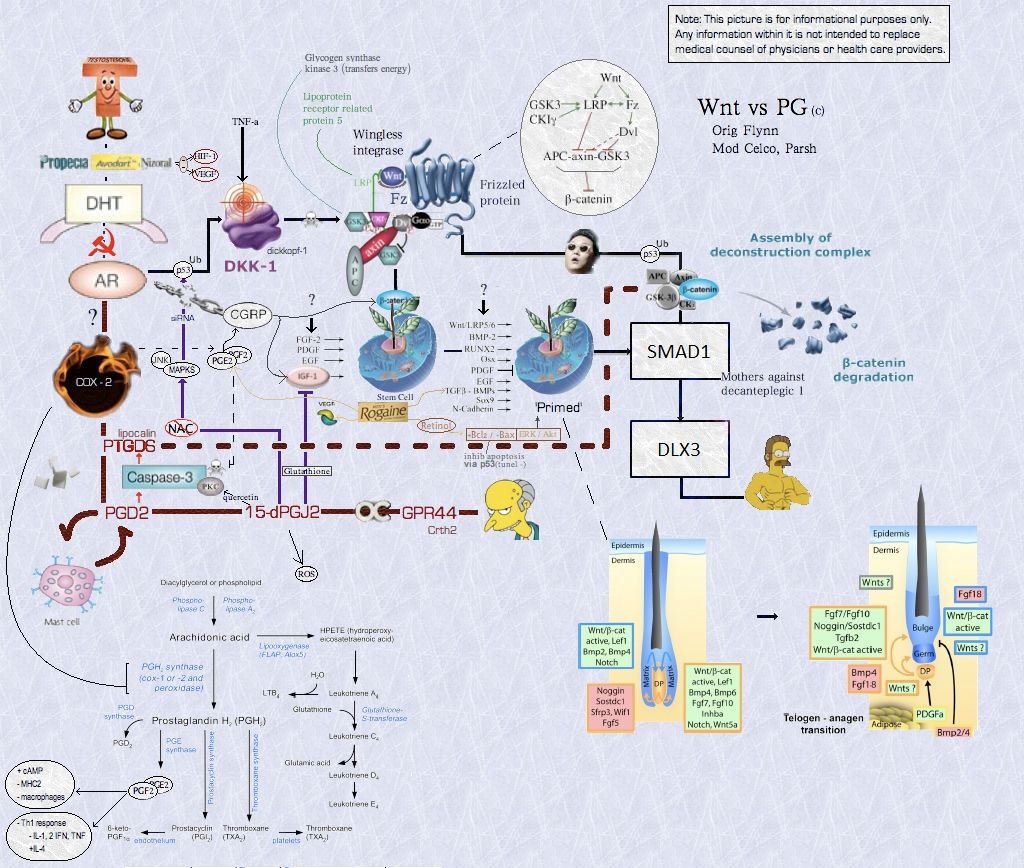
Top left next to the AR (androgen receptor) , P53. Things are starting to break down from there is my assumption. After reading many studies I am pretty certain, actually almost 100% that the WNT pathway is involved too. Instead of looking to Alopecia areata (AA) we should look to a disease which has more similarities to androgenetic alopecia. A disease which comes way closer than AA is hypotrichosis simplex. The miniaturization has extremely many comparisons to androgenetic alopecia (sparse thin hair). Now in hypertrichosis simplex they found a gene responsible for it;
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3046868/.
http://blog.americanhairloss.org/hai...s-gene-apcdd1/
APCDD1! The patent for it from A.M Christiano;
http://www.google.com/patents/US20120003244
So now you guys are asking wtf we ain't suffering from hypotrichosis simplex?! Yes but the similarities to androgenetic alopecia are unlike any other disease. So because of this discovery researchers in february took it one step further and checked if there was any association between this gene and androgenetic alopecia.
And guess what? Jup. They found an association; http://www.davidpublishing.com/david...0405863307.pdf.
In summary, our results demonstrated that the
synonymous rs3185480 polymorphism of the
APCDD1 gene is associated with the development of
the most common hair disorder, AGA
Another study which points out genetic evidence of the WNT pathway ; http://www.nature.com/jid/journal/v1...id201343a.html. Btw APCDD1 obliterates WNT pathway if that wasn't clear by now.
Again the WNT pathway plays a huge immense role in AGA, and I think anyone who reads papers HAS to agree on this one. There points way, way to much evidence for this.
Back to P53, as Parsh pointed out in the diagram I think that is where things start to fall apart. A quick paper for P53 evidence in the scalp; http://www.ncbi.nlm.nih.gov/pubmed/18702626. Basically P53 is overexpressed in bald scalp vs non-aga and occipital scalp.
P53 completely obliterates WNT signalling and induces DKK-1 (http://www.ncbi.nlm.nih.gov/pubmed/17657240) ;
- http://www.nature.com/nrm/journal/v1...l/nrm3238.html
- http://www.ncbi.nlm.nih.gov/pubmed/10777218
- http://www.ncbi.nlm.nih.gov/pubmed/22045851
P53 on it's own can already stop cell profileration though, this is done by activating P21 which in turn binds to Cdk/cyclin complex and this in turn will stop cell division.
https://www.youtube.com/watch?v=0klARAxOYiI
Watch the movie he basically researches the same, this was at the hair congress this year which desmond has recorded!
Anyways I'll stop here lol, I can go way deeper but that isn't necessary hopefully you guys get a idea what i think is somewhat happening in AGA. Can't be specific obviously but in the broad terms I think that is where things start to get fcked literally.
Forget to point out that P53 and PGD2 share the same regulators.
Ohw btw and LASTLY a very recent discovery to hypothricosis simplex too; http://www.nature.com/ng/journal/v40/n3/full/ng.84.html
Hypotrichosis simplex is a group of nonsyndromic human
alopecias. We mapped an autosomal recessive form of this
disorder to chromosome 13q14.11–13q21.33, and identified
homozygous truncating mutations in P2RY5, which encodes an
orphan G protein–coupled receptor. Furthermore, we identified
oleoyl-L-a-lysophosphatidic acid (LPA), a bioactive lipid, as a
ligand for P2Y5 in reporter gene and radioligand binding
experiments. Homology and studies of signaling transduction
pathways suggest that P2Y5 is a member of a subgroup of LPA
receptors, which also includes LPA4 and LPA5. Our study is
the first to implicate a G protein–coupled receptor as essential
for and specific to the maintenance of human hair growth.
This finding may provide opportunities for new therapeutic
approaches to the treatment of hair loss in humans.
Obviously A.M Christiano found this out again :") http://www.google.com/patents/US20140134188
Somebody better e-mail her that she starts investigating AGA soon!  . .
-
Woah im speechless... So much information. Swooping you are a wise man  keep it coming! keep it coming!
I dont think its caused by autoimmune thingy either. Fast forward "aging" sounds right because as an example: Nowdays women start to get their periods at earlier age than 100 years ago (better nutrition is thought to speed up the process). So maybe the same thing is happening to males too? Something is speeding up the part of the aging process and ****s up things.
Some people bald very slowly so if MPB is an autoimmune response i would think it should happen faster. AA happens fast.
Also seborrea, rosacea and psoriasis are linked to MPB somehow i think, since these diseases are common in men with MPB.
-
Btw about homeless alcoholics I think this leads really to a simpler conclusion. Alcohol really messes with the hormonal balance http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3258349/;
Results
Acute alcohol administration resulted in changes in gonadal hormones that differed by sex. Change in free testosterone showed a significant treatment × baseline interaction (p<0.001), indicating that alcohol-induced suppression of testosterone occurred predominantly in males, On the other hand, change in estradiol showed a significant treatment × sex interaction (p=0.028), indicating that alcohol-induced increases in estradiol occurred predominantly in females. There was a trend for alcohol-induced decreases in IGF-1 levels. Change in GH showed a significant main effect of baseline (p<0.001) and a trend for treatment by baseline interaction, suggesting an alcohol-induced decrease in individuals with high baseline GH values. There was also a significant main effect of sex (p=0.046) indicating that males had greater changes in GH across treatment compared to females.

These are pretty significant changes, estradiol obviously has a huge positive effect on hair. Lowering free test is extremely good. It has been proven many times that people with low SHBG values and high free test (FML lol) are the guys who bald extremely fast and aggressive. Alcohol also has effect on igf-1 and GH, both play a part in hair follicle function too.
If you would be drinking alcohol 24/7 that will literally change your HTPA axis (hormones) which will probably be beneficial for your hair yes. After all it is a polygenic inheritance so environmental factors play a role too. Eating soy 24/7 will probably hold your hair too, you might regrow even some and grow some boobs and a vagina with it (http://www.plosone.org/article/info%...l.pone.0079789).
All in all I think that would be the cause of alcoholics having a less incidence of hair loss.
-
Originally Posted by hairbackpls
Woah im speechless... So much information. Swooping you are a wise man keep it coming!
I dont think its caused by autoimmune thingy either. Fast forward "aging" sounds right because as an example: Nowdays women start to get their periods at earlier age than 100 years ago (better nutrition is thought to speed up the process). So maybe the same thing is happening to males too? Something is speeding up the part of the aging process and ****s up things.
Some people bald very slowly so if MPB is an autoimmune response i would think it should happen faster. AA happens fast.
Also seborrea, rosacea and psoriasis are linked to MPB somehow i think, since these diseases are common in men with MPB.
Yeah exactly. The DHT and subsequently the androgen receptor f*cks things up in our case. This is interesting too, just started reading it http://www.plosone.org/article/info%...l.pone.0031052. I think the androgen receptor says bye bye in our case and obviously starts the cascade leading to less proliferation and senescence, thus having miniaturized hair. The study points that out from what I understand now although it points out it is p53 independent. Let's break the study up;
AR proliferative effects rely on Cyclin D1 [7]; its survival effects involve Akt and anti-apoptotic proteins Bcl-2 and Mcl
I mentioned Cyclin before. Now AKT and bcl-2 are very important for hair growth, this has been pointed out in many papers.
Here we demonstrate that continuous AR activation in vitro and in vivo cause cellular senescence ( http://www.nature.com/nrm/journal/v8...l/nrm2233.html), which can be attenuated by AR antagonist, anti-androgen flutamide. Cellular senescence is one of the events underlying tumor suppression. Senescence can be triggered by telomere shortening or stress, including inappropriate expression of growth-promoting genes, GTPases or reactive oxygen species (ROS) [21]. Senescence can be driven by Rb or p53 pathways, which are closely intertwined: Rb can block p53-destabilizing protein MDM2, thus increase p53 levels, promoting the expression of p53 targets, p21, Bax and PIG3 and cause senescence [22], [23]. On the other hand, p21 inhibits cyclin dependent kinases (Cdks) and therefore dephosphorylates and activates Rb, which then binds E2F allowing the expression of growth arrest genes and senescence [22], [24].
As said basically AR activation in vivo and in vitro can cause cellular senescence. For example as I pointed out P53> P21> Cdk/Cyclin > arrest. Furthermore Bax is bad for our hair (pro-apoptic). Funny enough when using a androgen receptor antagonist (flutamide) they stopped the senescence. That's what we are doing also with RU58841 and soon CB-03-01, and some people use other anti-androgens.
Now let's look at minoxidil for a in vitro study http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2693596/.
The Bcl-2 family proteins are structurally related molecules that play an essential role in the regulation of apoptosis (27). Bcl-2 family consists of anti-apoptotic proteins such as Bcl-2 as well as pro-apoptotic proteins such as Bad and Bax. Erk and PI3K/Akt pathways synergistically induce cell survival by Bcl-2 cascade (28). Throughout the hair cycle, dermal papilla (DP) is the only region expressing consistently Bcl-2 proteins and the Bax proteins are not detected during hair cycles (
Minoxidil plus ATRA more increased the phosphorylation of Erk and Akt early 1 hr after the treatment than minoxidil alone. The change of Bcl-2/Bax ratio, P53 and P21 were also detected later 24 hr after the treatments. Minoxidil plus ATRA could work together to prolong the survival of cultured DPCs and epithelial cells and to protect them from apoptosis by dual mechanisms with different kinetics: 1) the activation of Erk- and Akt-dependent pathways and 2) the increase of the ratio of Bcl-2/Bax and the suppression of the expression of P53 and its downstream target P21.
Yeah! Minoxidil reduces P53 and subsequently (?) increases bcl2/bax ratio and induces ERK/AKT. Shown again in the diagram too by parsh though i think somewhere.
Researches very often screen for these markers to have an idea on the effectivity of compounds, a random example; http://www.plosone.org/article/info%...l.pone.0092984
Apoptosis with premature termination of hair follicle growth induces several types of hair loss and is one of the crucial factors of hair loss. Astragaloside IV, which is a major component of Astragalus membranaceus, is a cycloartane triterpene saponin. Although an anti-apoptotic effect of Astragaloside IV has been reported, its effects against hair loss have not been investigated. To explore the underlying mechanisms of Astragaloside IV on apoptotic signaling in hair follicle, the dorsal skin of depilated C57BL/6 mice was topically treated with 1 and 100 μM Astragaloside IV for 14 days. In Astragaloside IV-treated group, TUNEL-positive cells were reduced. We found that Astragaloside IV blocked the procaspase-8, resulting in the inhibition of caspase-3 and procaspase-9 activities. The changes were accompanied with down-regulation of Bax and p53, and up-regulation of Bcl-2 and Bcl-xL by Astragaloside IV treatment. In addition, activation of NF-κB and phosphorylation of IκB-α were inhibited, along with decreases in three MAPKs: ERK, SAPK/JNK and p38 by Astragaloside IV. The expressions of KGF, p21, TNF-α and IL-1β, which are keratinocyte terminal differentiation markers associated with catagen, were modulated by treatment with Astragaloside IV.
Another one ; http://www.ncbi.nlm.nih.gov/pubmed/24244503 Androgen receptor accelerates premature senescence of human dermal papilla cells in association with DNA damage
Androgen receptor accelerates premature senescence of human dermal papilla cells in association with DNA damage. The dermal papilla, located in the hair follicle, expresses androgen receptor and plays an important role in hair growth. Androgen/Androgen receptor actions have been implicated in the pathogenesis of androgenetic alopecia, but the exact mechanism is not well known. Recent studies suggest that balding dermal papilla cells exhibit premature senescence, upregulation of p16(INK4a), and nuclear expression of DNA damage markers. To investigate whether androgen/AR signaling influences the premature senescence of dermal papilla cells, we first compared frontal scalp dermal papilla cells of androgenetic alopecia patients with matched normal controls and observed that premature senescence is more prominent in the dermal papilla cells of androgenetic alopecia patients. Exposure of androgen induced premature senescence in dermal papilla cells from non-balding frontal and transitional zone of balding scalp follicles but not in beard follicles.Overexpression of the AR promoted androgen-induced premature senescence in association with p16(INK4a) upregulation, whereas knockdown of the androgen receptor diminished the effects of androgen. An analysis of γ-H2AX expression in response to androgen/androgen receptor signaling suggested that DNA damage contributes to androgen/androgen receptor-accelerated premature senescence. These results define androgen/androgen receptor signaling as an accelerator of premature senescence in dermal papilla cells and suggest that the androgen/androgen receptor-mediated DNA damage-p16(INK4a) axis is a potential therapeutic target in the treatment of androgenetic alopecia.
Btw I would like to point out that anyone suffers from this even a tiny bit. Who still has their hair at the age of 80 just as they had it when they were 18? Even non-AGA people will notice a decline in follicular anagen state, less density, less thick hair and greying ; http://www.ncbi.nlm.nih.gov/pubmed/24033376
One key issue that is in common to these processes is oxidative damage. At the hair follicle stem cells niche, oxidative stress, accelerated by B-cell lymphoma 2 gene (BCL-2) depletion, leads to selective apoptosis and diminution of melanocyte stem cells, reducing the repopulation of newly formed anagen follicles. Melanotic bulbar melanocytes express high levels of BCL-2 to enable survival from melanogenesis- and ultraviolet A (UVA)-induced reactive oxygen species (ROS) attacks. With ageing, the bulbar melanocyte expression of anti-oxidant proteins such as BCL-2, and possibly TRP-2, is reduced, and the dedicated enzymatic anti-oxidant defence system throughout the follicle weakens, resulting in enhanced oxidative stress.
Yes everyone gets attacked by it. But DHT in our case completely f*cks us up. Why the pattern though? Why do some bald in the crown like but has a perfect hairline? Why do some only develop to NW2 at age 50 without treatments? Is it that simple of increased androgen receptor expression like pointed out in studies? Or is it because of higher sensitivity of the AR co-receptors at our hair follicle as pointed out by another study? Or... Well there are still many questions to be solved I guess.
This also shows why AGA is so extremely difficult to handle, unlike AA.
-
Holy ****! you are a machine. You will figure it out soon, bro i believe in you.
Yeah the pattern is a mystery. Humans sweat most from the MPB area and lose 90% of the body heat through the scalp.
I also think that drugs that reduce sebum and sweatting could help since MPB sufferers hair gets greasy very fast (myself as an example.. My hair is full of hardened sebum balls when ive been sweatting alot and skipped a day in showering). Women sweat less and has less oily hair. Someone could try Oxybutynin. None bad side effects so nothing to lose.
Btw i think that acne is linked to this same process since i never had acne before my hairloss started... AND most people didint have acne 100 years ago (look at old pictures). Hairloss wasnt so common back then either and it started at later age.. Something ****s up the process and causes these things.
Similar Threads
-
By clandestine in forum Coping with Hair Loss in Everyday Life
Replies: 42
Last Post: 01-26-2015, 04:24 AM
-
By baldozer in forum Hair Transplant: Start Your Own Topic
Replies: 19
Last Post: 05-17-2014, 02:41 PM
-
By Artha in forum Men's Hair Loss: Start Your Own Topic
Replies: 0
Last Post: 05-16-2014, 02:55 PM
-
By JFols in forum Coping with Hair Loss in Everyday Life
Replies: 3
Last Post: 05-15-2013, 02:26 PM
-
By gmonasco in forum Men's Hair Loss: Start Your Own Topic
Replies: 0
Last Post: 04-04-2012, 09:12 PM
 Posting Permissions
Posting Permissions
- You may not post new threads
- You may not post replies
- You may not post attachments
- You may not edit your posts
Forum Rules
|
» IAHRS
» The Bald Truth
» americanhairloss.org
|



 Reply With Quote
Reply With Quote


")

Bookmarks