-
-
'Fingers' are CERTAINLY *crossed* Javert ...
When I finally met with Dr Wesley in person last month, his sincerity in what he is doing and working on was quite obvious!Comment
-
I am trying to participate in the trial as well...have an appointment coming up and will see.Comment
-
Dr. Wesley,
It sounds like you're saying that you intend to go under the skin and remove follicles from underneath while also leaving behind some tissue for each harvested follicle and you hope that the tissue left behind plus ACELL will regenerate new follicle in place of the harvested follicles. Even if this is possible how can you be sure that your machine can harvest the follicles from underneath at the exact right spot on the follicle so that you harvest enough of the follicle to grow after implanted to the thinning area while also leaving behind enough of that same follicle to regenerate? It sounds to me like you are going to have to severe the follicle at a very specific spot on the follicle and I don't see how you can achieve this coming to the follicle from below the skin where you can't even see the follicle. How can you severe the follicle at the exact right spot when you can't even see it? Also we are not talking about harvesting a single follicle - we are talking about harvesting many many follicles. How are you going to harvest many many follicles, severing them all at the exact right location on each follicle, under the skin when you can't even see where you are cutting?
2. I do not have high confidence in ACELL at all. If Acell could regenerate harvested follicles then this would already be widespread globally throughout the hair transplant industry. A lot of doctors have tried regeneration of donor tissue using Acell and as far as I know nobody has succeeded. If Clooney had really pulled it off then the entire hair transplant industry would be using Acell to regenerate donor follicles after harvesting donor follicles and it would be big news in the media. A successful donor regeneration after harvesting donor follicles would be a BIG story.Comment
-
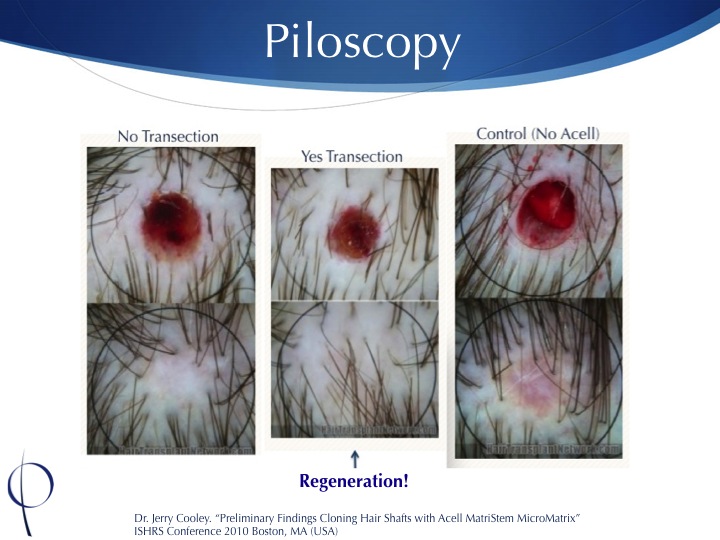
Dr. Wesley discussed this in his last call with Spencer. It's a very small space to hit, and very small adjustments may need to be made to hit this spot as it differs between people. I believe Dr. Wesley stated that maybe taking a few out with FUE initially to see this depth and adjust could be an option (not 100% sure I'm recalling this correctly, you can watch the video though). However, finding an average depth to extract the follicles, while leaving the upper portion in it's original environment may be all that is needed. Dr. Wesley seemed to suggest in the phone call that he believed keeping the follicle in it's original environment was more important than what Acell could do for any regeneration. If you have read the study he posted, they split the follicles horizontally and implanted both ends on balding scalp (a much more harsh environment then where one portion of the follicle would stay in the donor zone) and both halves grew with an average of 75% yield. The idea is, if one half is staying in the donor region where it's in it's original environment, maybe we can increase that 75% for that half. Further, maybe adding things like PRP/Acell can help both halves increase their yield. I don't think it takes a rocket scientist to see how Piloscopy could improve upon the technique used in this study that clearly worked for multiplying follicles.
Furthermore, Dr. Cooley has presented clear evidence that it works to some extent, and this is backed up by Dr. Cole who sees regeneration in his clinic all the time to various degrees. Dr. Cole stated the only problem is, the ACell leaks from the extracted follicle site where they need it to stay to do it's job and that's why he is seeing a great range of inconsistent regeneration rates. However, if you are flooding the donor area with Acell under the skin, where you are extracting the follicles, then there is nowhere for it to leak. I think that's another obvious reason Piloscopy has so much potential. However, regardless of if ACell works, my impression was Dr. Wesley believes the half of the follicle staying in the original atmosphere is far more important. I guess time will tell.
Artista, have you set your date yet for your phase testing? or has Dr. Wesley resumed this? Lastly, do you have any idea of when he plans to be doing large sessions (2000 grafts+) and begin using this in his practice?Comment
-
Dr. Wesley discussed this in his last call with Spencer. It's a very small space to hit, and very small adjustments may need to be made to hit this spot as it differs between people. I believe Dr. Wesley stated that maybe taking a few out with FUE initially to see this depth and adjust could be an option (not 100% sure I'm recalling this correctly, you can watch the video though). However, finding an average depth to extract the follicles, while leaving the upper portion in it's original environment may be all that is needed. Dr. Wesley seemed to suggest in the phone call that he believed keeping the follicle in it's original environment was more important than what Acell could do for any regeneration. If you have read the study he posted, they split the follicles horizontally and implanted both ends on balding scalp (a much more harsh environment then where one portion of the follicle would stay in the donor zone) and both halves grew with an average of 75% yield. The idea is, if one half is staying in the donor region where it's in it's original environment, maybe we can increase that 75% for that half. Further, maybe adding things like PRP/Acell can help both halves increase their yield. I don't think it takes a rocket scientist to see how Piloscopy could improve upon the technique used in this study that clearly worked for multiplying follicles.
Furthermore, Dr. Cooley has presented clear evidence that it works to some extent, and this is backed up by Dr. Cole who sees regeneration in his clinic all the time to various degrees. Dr. Cole stated the only problem is, the ACell leaks from the extracted follicle site where they need it to stay to do it's job and that's why he is seeing a great range of inconsistent regeneration rates. However, if you are flooding the donor area with Acell under the skin, where you are extracting the follicles, then there is nowhere for it to leak. I think that's another obvious reason Piloscopy has so much potential. However, regardless of if ACell works, my impression was Dr. Wesley believes the half of the follicle staying in the original atmosphere is far more important. I guess time will tell.
Artista, have you set your date yet for your phase testing? or has Dr. Wesley resumed this? Lastly, do you have any idea of when he plans to be doing large sessions (2000 grafts+) and begin using this in his practice?Comment
-
Really great technique, I hope that it will not take a too long time before being avalaible for us
When larger sessions will be possible with piloscopy, even a Nwd 6 could have an option: take a maximum of grafts in the donor area( 6000,8000, or even more) to put on the top. And then do smp on sides and back to fill the gaps where's there no hair.
Like that he could grow his hair on top with decent density, and shave on sides and back. Okay he will have just one haircut option, but it's a better one than the horseshoe one in my opinion ^^
And for the minor Norwood, it will be better than fut/fue tooComment
-
Artista it is basically July... Any word or updates on where Dr. Wesley is with his phase testing?Comment
-
The piloscope is now ready for limited clinical use in a select group of patients. Development and testing of the device that enables select harvesting of the stem-cell containing portion of hair follicles without traumatizing the overlying skin surface has led us to this point. The company (Pilofocus) overview can be seen here.
Beginning at the end of July 2015, a handful of patients will be able to undergo very limited surgical hair restoration with this method. The cases will initially involve transplantation of approximately 100-200 follicular units. Although this "scarless surgical" method will eventually be made available to all hair types, patients most suitable for the initial piloscopic procedures are those who have previously undergone follicular unit transplantation (FUT) as the instrument will harvest donor hair adjacent to their donor scar. There is no charge for patients selected to take part in these initial, small pilosocpic procedures.
Please email, Barbara, our office manager at info@drcarloswesley.com or call 844-PILOFOCUS (1-844-745-6362) for more information.Carlos Wesley, MD
Member, International Alliance of Hair Restoration Surgeons
View my IAHRS Profile
1050 Fifth Avenue
New York, NY 10028
844-745-6362
http://www.drcarloswesley.com
info@drcarloswesley.com
Comment
-
I was waiting for age 35 to see if my hairloss would have sped up or if Finasteride would maintain before getting a transplant. I think with PiloFocus I can do it earlier because there's no risk of an FUT scar if I must shave my head later, say after age 50 in ~20 years time.Comment
-
Wow Dr. Wesley you're God!
Thanks for your update!Comment

 Tweet
Tweet





.pdf)



Comment