I'm going to start off by stating that plasma DHT levels are a very inconsistent measure for the battle against hair loss, for several reasons. The quantities of DHT found in the blood are more or less pointless, since they are leftovers that have leaked from autocrine reduction on target tissue. What this means is, plasma DHT levels are a byproduct of either too few androgen receptors near the local site in which they are produced, or a high 5-AR activity that has caused over-saturation of androgen receptors and thus excess quantities are released in the bloodstream. This is why serum DHT levels do not really mean anything, they are a proxy measure for the enzyme inhibition of finasteride at best.
Finasteride is not only an inhibitor of 5-ar II enzymes, it's a suicide inhibitor. Meaning that once finasteride binds to a 5-ar enzyme, BOOM, it's gone. It forms an irreversible bond forever. So even though the half life of finasteride is only 6 hours, it takes up to a week for serum DHT levels to get to baseline after a single dose. The reason for that is, the half life turnover rate of the 5-αr II enzyme is somewhere between 15 to 30 days. Generally, the amount of finasteride you take and the frequency in which you take it is generally irrelevant on a broad scale, seeing as it can be effective from doses as low as 0.12mg, and it takes probably at least 72 hours to have any appreciable change on serum DHT.
But there's a catch, I've already mentioned that serum DHT levels means little for hair loss. Over 75% of serum DHT levels are originated from the prostate, since it's responsible for about 60% of total DHT levels in the body alone. So if anything, the serum DHT levels would a proxy measure for amount of DHT bounded by androgen receptors on prostate tissue. But if you are not medicating finasteride to relieve benign prostatic hyperplasia, then that is highly irrelevant. Most of us are more interested in it's mechanism for slowing down hair loss.
Finasteride is not that effective in inhibiting scalp homogenate 5-alpha-reductase activity using micro doses. The general consensus on the efficacy of finasteride comes from the fact that it fights against MPB by blocking DHT conversion inside the hair follicle. That is the whole essence of 5-AR inhibitors, and the reason why they work. The bigger factor at work here is potency with respect to the scalp. Since the scalp has lower blood circulation and fewer concentrations of 5-AR enzymes than the prostate, it would naturally take a much higher concentration to give the same effects as it would for the prostate. Having said that, the IC50 of finasteride for prostate and scalp homogenates was reported to be 5.9 and 310 nM, respectively on average, consistent with other numerous attempts of measure. With this in mind, it was estimated that a concentration of 94 nM finasteride would inhibit prostate homogenate 5-AR activity by 85%, but would inhibit scalp homogenate 5-AR activity by 25%. An early MERCK study showed that value closer to 32% if I recall correctly. So by extrapolation, in order to achieve a level of inhibition in scalp tissue that was comparable to that in the prostate, the concentration of finasteride in plasma would have to be around 1 uM, which would be obtained following a single oral 50 mg dose of finasteride. So again, if you want maximal DHT inhibition inside follicular tissue, you would need doses in excess of 15 mg everyday. But seeing as reductions as little as 25% was enough to stop androgenic tissue expression for hair miniaturization, that would be unnecessary.
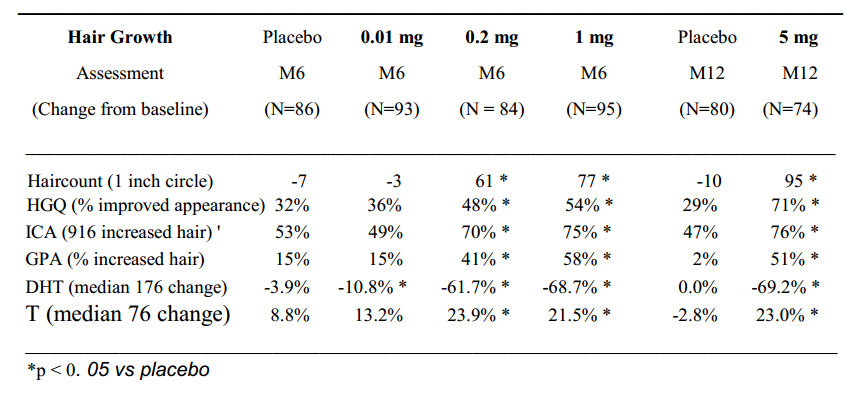
Again, consistent with these findings, hair counts seem to improve by increasing daily doses of finasteride.
The conclusion I have reached at reaching the best possible dose-result ratio schedule would be somewhere around 0.5mg to 1.0mg everyday.



 Reply With Quote
Reply With Quote
 . At times I can pull my hands through my hair and nothing will come out and at other times maybe only one or two and in the shower I can run my hands through my hairs and end up with under four hairs every time. In comparison before starting my treatment pulling my hands through my hair would result in plus five hairs coming out every time and running my hands through my hair in the shower could see me at times end up pushing 10 - 15 hairs.
. At times I can pull my hands through my hair and nothing will come out and at other times maybe only one or two and in the shower I can run my hands through my hairs and end up with under four hairs every time. In comparison before starting my treatment pulling my hands through my hair would result in plus five hairs coming out every time and running my hands through my hair in the shower could see me at times end up pushing 10 - 15 hairs. 



")
Bookmarks